
“Trauma changed my brain forever.”
This phrase has become a common refrain… appearing in social media posts, movie dialogue, and everyday conversations.
While it reflects the depth of emotional suffering, it can also unintentionally suggest that trauma leaves a person permanently ‘broken’ and beyond healing.
In truth, trauma may alter the brain, but it does not irreparably damage it.
Modern neuroscience demonstrates that the brain is remarkably resilient and capable of adaptation.
Understanding this helps dismantle a damaging myth and brings hope to countless people on their journey toward recovery.
Trauma is defined as an emotional response to profoundly distressing or life-threatening events, including abuse, accidents, natural disasters, violence, or the sudden loss of a loved one.
Although these events can leave lasting psychological effects, not everyone who experiences trauma develops a mental health disorder.
In fact, resilience is common, and many individuals experience natural recovery over time.
What Happens to the Brain After Trauma
When trauma occurs, the brain activates its survival system, commonly known as the ‘fight, flight, or freeze’ response.
This process involves several critical brain regions.
The amygdala, which acts as the brain’s alarm system, becomes highly active, increasing feelings of fear and alertness; the hippocampus, which processes and contextualises memories, may experience structural or functional changes, contributing to intrusive or fragmented recollections; and the prefrontal cortex, which helps regulate emotions and supports clear thinking, can become less active, making it harder to cope with intense emotional reactions.
These changes in the brain can explain why people who have experienced trauma may feel constantly on alert, have trouble focusing, or relive distressing memories.
However, it is important to emphasise that these changes are adaptive rather than inherently damaging.
They represent the brain’s natural effort to protect the individual from future danger.
Importantly, evidence suggests that many of these changes can be reversed, particularly with adequate psychological and social support.
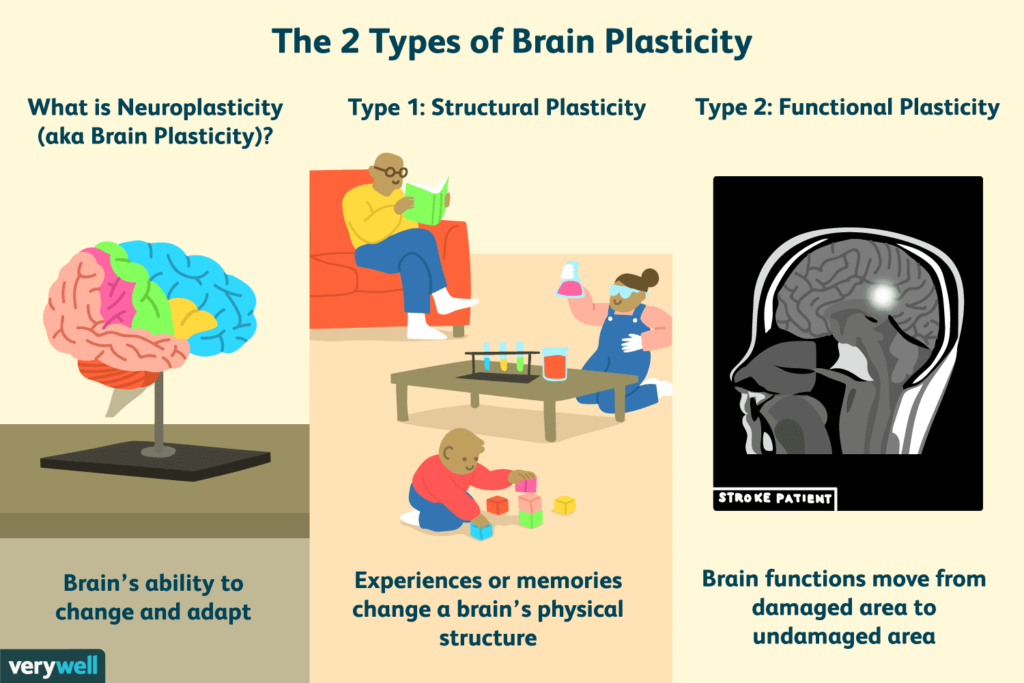
Neuroplasticity: The Brain’s Built-In Resilience
This recovery is made possible by neuroplasticity, which is the brain’s ability to reorganise itself by forming new connections throughout life.
This allows the brain to adapt, learn, and recover from adversity.
In other words, the brain is not fixed; it is constantly changing and reshaping itself.
Research using neuroimaging has shown that the brain can positively respond to effective treatments for trauma-related disorders.
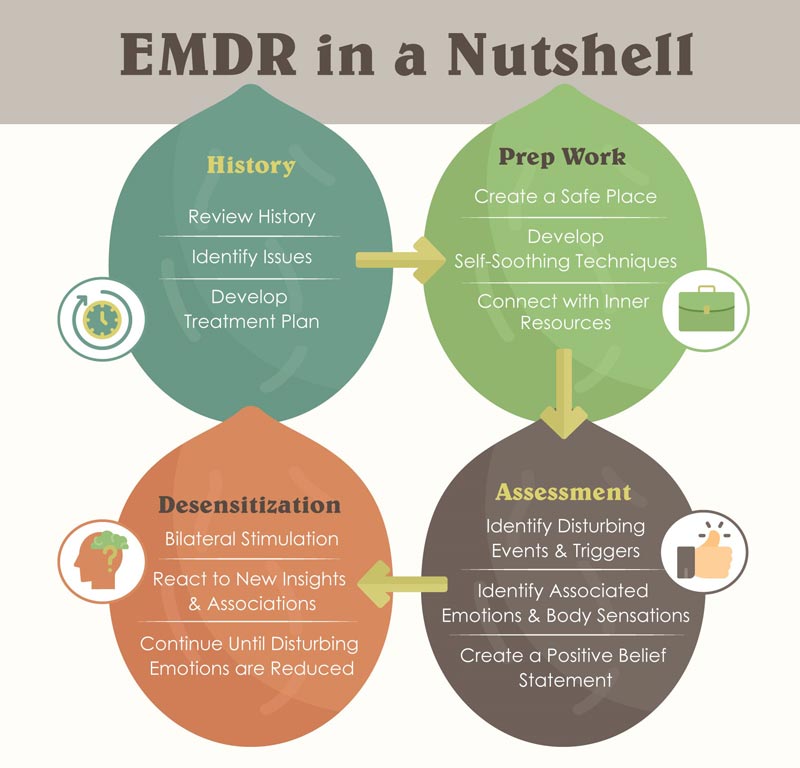
For example, trauma-focused cognitive behavioural therapy (TF-CBT) and Eye Movement Desensitisation and Reprocessing (EMDR) have been found to normalise amygdala activity and strengthen prefrontal cortex functioning, thereby enhancing emotional regulation.
These findings strongly indicate that the brain retains the ability to heal and adapt even after experiencing profound psychological distress.
In other words, the brain that learns to survive trauma is also capable of learning to heal.
Trauma and Mental Health: An Invisible but Common Struggle
Although trauma is a common human experience, it does not always lead to a diagnosable mental illness.
However, such exposure significantly increases the likelihood of developing mental health conditions.
Notably, depressive and anxiety disorders are the most prevalent outcomes of trauma, occurring more frequently than Post-Traumatic Stress Disorder (PTSD).
Understanding this range of trauma-related conditions helps challenge misconceptions and encourages individuals to seek the support they need.
Post-Traumatic Stress Disorder (PTSD)
Among trauma-related conditions, Post-Traumatic Stress Disorder (PTSD) is the most widely recognised.
Global estimates suggest a lifetime prevalence of roughly 3–4% in the general population, with significantly elevated rates among individuals exposed to prolonged or high-intensity trauma.
The symptoms of PTSD are generally organised into four key clusters:
- Intrusion: Repeated and distressing memories or dreams in which the traumatic event is relived.
- Avoidance: Attempts to stay away from people, places, thoughts, or feelings that bring back memories of the trauma.
- Negative Changes in Mood and Cognition: Persistent negative emotions, such as guilt or shame, and a sense of disconnection from others.
- Hyperarousal: A constant state of alertness, often resulting in irritability, difficulty sleeping, and being easily startled.
These symptoms can disrupt daily life; however, they are highly treatable with proper care.
Other Trauma-Related Mental Illness
Acute Stress Disorder (ASD)
Acute Stress Disorder (ASD) occurs during the first month following a traumatic experience.
Although it shares many clinical features with Post-Traumatic Stress Disorder (PTSD), it is generally less prevalent and often resolves without long-term consequences.
Prevalence rates are estimated to range from 5% to 20%, influenced by the type and severity of trauma.
While some individuals with ASD may later develop PTSD, many recover without progressing to it.
Complex Post-Traumatic Stress Disorder (C-PTSD)
Complex Post-Traumatic Stress Disorder (CPTSD), recognised in the ICD-11, is associated with exposure to persistent or repetitive trauma, particularly interpersonal in nature, such as childhood abuse or domestic violence.
In addition to the symptoms associated with PTSD, individuals may also experience:
- Difficulty understanding and managing intense emotions
- Feeling fundamentally flawed or inadequate
- Difficulty building or sustaining meaningful connections
Although clinically significant, C-PTSD is generally less prevalent in the general population compared to PTSD.
Dissociative Disorders
Among the rarer trauma-related conditions are dissociative disorders, including Dissociative Identity Disorder (DID).
These disorders are strongly connected to experiences of severe and long-term trauma, especially during early childhood.
Prevalence estimates indicate that these disorders affect less than 1% of the general population, making them relatively rare compared to other trauma-related mental illnesses.
Causes and Risk Factors
The likelihood of developing trauma-related mental health conditions depends on a combination of biological, psychological, and social factors.
Key risk factors include:
- The severity and length of the traumatic experience
- Childhood adversity
- Limited social support
- Pre-existing psychological conditions
- Genetic risks
- Ongoing life stress
In contrast, protective factors such as strong interpersonal relationships, access to mental health services, and effective coping strategies play a crucial role in enhancing resilience and promoting recovery.
Adapting to Trauma: A Shift from Repair to Resilience
Recovery from trauma is not about erasing the past or reverting to a pre-trauma self.
Rather, it typically involves adaptation and integration, whereby individuals learn to construct meaningful lives while recognising and processing the impact of their experiences.
Evidence-Based Practices in Trauma Recovery
- Psychological Therapies
- Trauma-Focused Cognitive Behavioural Therapy (TF-CBT)
- Eye Movement Desensitisation and Reprocessing (EMDR)
These treatments facilitate the processing of traumatic memories while enhancing the individual’s ability to regulate emotional responses.
- Medication
- Selective serotonin reuptake inhibitors (SSRIs) are a commonly prescribed class of medication for conditions such as PTSD, depression, and anxiety.
- Social Support
- Strong interpersonal relationships offer emotional validation and promote a sense of safety, thereby significantly enhancing recovery outcomes.
- Mind–Body Practices
- Practices such as mindfulness, yoga, and regular exercise can help improve emotional regulation and lower the body’s stress responses.
Post-Traumatic Growth: Pathways to Positive Change After Adversity
An important part of recovering from trauma is the idea of post-traumatic growth.
Rather than simply returning to pre-trauma levels of functioning, some individuals experience positive psychological changes following adversity.
These may include:
- A renewed sense of gratitude for life
- Improved connection with family and friends
- Improved ability to withstand adversity
- Strengthened life purpose and direction
While not everyone experiences post-traumatic growth, it demonstrates the human capacity for transformation in the face of adversity.
Why This Misconception Needs to Be Addressed?
It is important to correct the misconception that trauma irreversibly damages the brain, as this belief can increase stigma and discourage individuals from seeking help.
When people internalise the belief that they are permanently “broken,” it can lead to hopelessness and withdrawal from treatment.
In contrast, recognising the brain’s neuroplasticity promotes empowerment, hope, and resilience.
In the current digital era, where mental health narratives spread rapidly through social media platforms, it is important to balance emotionally compelling storytelling with scientific accuracy.
While phrases like “trauma changed my brain forever” are powerful and relatable, they should be reframed to focus on adaptation and healing rather than permanent damage.
A Message of Hope for Young People
Ultimately, scientific evidence demonstrates that the brain is not a fragile structure that breaks under stress, but a highly adaptable organ capable of profound transformation.
Neuroplasticity allows the formation of new pathways that support healing, meaning individuals can not only recover but also grow in meaningful ways.
For young people navigating mental health challenges, this offers an important message of hope.
Trauma may form part of an individual’s life narrative, but it does not define its conclusion.
With appropriate intervention, knowledge, and supportive environments, recovery is not only possible but anticipated.
References:
American Psychiatric Association. (2019). Summary of the clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. https://doi.org/10.1037/amp0000473
Bonanno G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events?. The American psychologist, 59(1), 20–28. https://doi.org/10.1037/0003-066X.59.1.20
Bremner, J. D. (2006). Traumatic stress: effects on the brain. Dialogues in Clinical Neuroscience, 8(4), 445–461. https://doi.org/10.31887/DCNS.2006.8.4/jbremner
Bryant, R. A. (2017). Acute stress disorder. Current Opinion in Psychology, 14, 127–131. https://doi.org/10.1016/j.copsyc.2017.01.005
Cleveland Clinic. (n.d.). Amygdala. https://my.clevelandclinic.org/health/body/24894-amygdala
Hayes, J. P., Hayes, S. M., & Mikedis, A. M. (2012). Quantitative meta-analysis of neural activity in posttraumatic stress disorder. Biology of Mood & Anxiety Disorders, 2(1), 9. https://doi.org/10.1186/2045-5380-2-9
Kessler, R. C., Berglund, P., Demler, O., Jin, R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
Koenen, K. C., Ratanatharathorn, A., Ng, L., et al. (2017). Posttraumatic stress disorder in the World Mental Health Surveys. Psychological Medicine, 47(13), 2260–2274. https://doi.org/10.1017/S0033291717000708
Malejko, K., Abler, B., Plener, P. L., & Straub, J. (2017). Neural correlates of psychotherapy in post-traumatic stress disorder: A systematic literature review. Frontiers in Psychiatry, 8, 85. https://doi.org/10.3389/fpsyt.2017.00085
Şar, V. (2011). Epidemiology of dissociative disorders: An overview. Epidemiology Research International, 2011, 404538. https://doi.org/10.1155/2011/404538
Tedeschi, R. G., & Calhoun, L. G. (2004). Posttraumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15(1), 1–18. https://doi.org/10.1207/s15327965pli1501_01
World Health Organization. (2019). International Classification of Diseases 11th Revision (ICD-11). World Health Organization.


{kind=link}